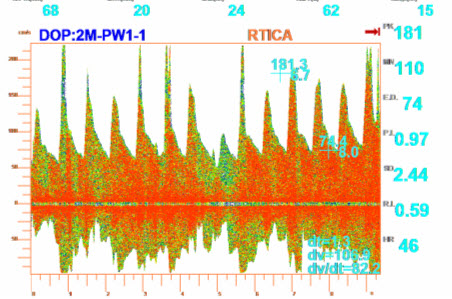
This example is of a stenotic right
terminal internal carotid artery,
insonated via the orbital window.
This is one of the most under
diagnosed forms of disease that
leads to stroke, because of technical
limitations of other neuro imaging
techniques.
 The most important
The most important
diagnostic criteria here is a mean
flow velocity greater than 80 cm/sec.
This example has a MFV of 110
cm/sec
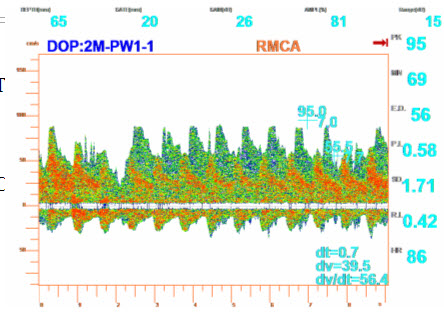
The below example is a right MCA with an ipsolateral ICA occlusion. In ICA occlusions evaluation of the intracranial arteries via TCD is vital because it show the physiological hemodynamics of the collaterals. In this case you can clearly see two wave forms above the base line. The smaller wave for is the MCA, the higher systolic peaked wave form is the active anterior communicating artery, cross filling left anterior circulation to right anterior circulation. This is an ideal example of the benefits of evaluating the intracranial arteries distal to disease with TCD. Neurological events will most probably be in direct correlation with collateral flow or the lack of.
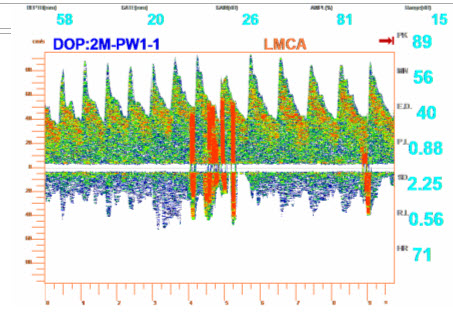
The final example is of a positive PFO study. The best results come after an injection of 9cc saline, one cc air, immediately followed by a 5-10 second gauged valsalva maneuver. In the case of a positive study air emboli will be observed with in seconds. This test is not performed with a head frame, just my hand, the probe and the assistance of a nurse for injecting. The audible sound is unmistakable and eliminates the possibility of artifact. Recent studies suggest the PFO test performed by TCD is more sensitive than TEE, which also means all positive PFO studies performed by TCD will not be confirmed by TEE. The only two ways the agitated saline can go from vein to MCA is, most probably PFO and secondly a pulmonary shunt. Their is no way to differentiate definitively the difference in pulmonary and right to left shunts with TCD. The gauged valsalva maneuver is essential to conduct this study with any degree of success.